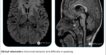
TRANSSPHENOIDAL MENINGOCELE


Clinical Information: Headache.
Findings:
Lobulated non-enhancing CSF signal intensity lesion seen anterior to the dorsum sella projecting into the sphenoid sinus and nasopharynx through a large craniopharyngeal canal.
There is a communication between the anterior recess of the third ventricle and the above mentioned lesion.
The pituitary stalk and gland can’t be identified.
– Possibility of transsphenoidal meningocele.
Distal most part of splenium of corpus callosum is not visualized -? Agenesis.
There is increased anteroposterior diameter of the eye globe on right site with focal deformity uveal outpouching at posterior aspect – possibility of staphyloma.
Discussion:
Cephaloceles occur in approximately one of every 3000 to 5000 live births. Classification into frontal, occipital, parietal, and basal.
Basal meningoencephaloceles, which occur with an estimated incidence of one in every 35,000 live births have been further subdivided, depending on the location of the bone defect, into transethmoidal, sphenoethmoidal, spheno-orbital and transsphenoidal .
The transsphenoidal type represents less than 5% of all basal meningoencephaloceles and has an estimated incidence of one in 700,000 live births.
Two types of transsphenoidal meningoencephaloceles:
1) The intrasphenoidal and 2) The true transsphenoidal.
Clinical presentation may include CSF rhinorrhea; visual impairment, most notably visual field defect, decreased visual acuity, amaurosis, or amblyopia; endocrine dysfunction, especially hypogonadism, hypothyroidism, hyperprolactenemia or diabetes insipidus and cranial facial defects, mostly hypertelorism.